0 CME
CME
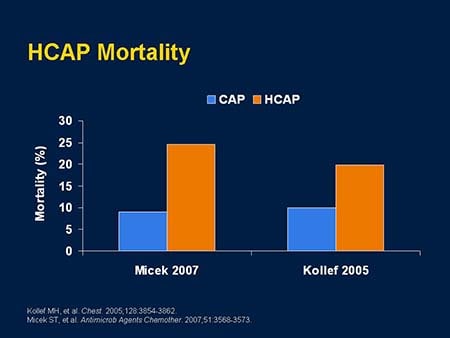
Critical Decisions for the Treatment of Health-care-Associated Pneumonia in the ICU
- Authors: Lee Morrow, MD, FCCP
- THIS ACTIVITY HAS EXPIRED FOR CREDIT
THIS ACTIVITY HAS EXPIRED FOR CREDIT

This activity is designed for physicians involved in the care of patients in the ICU.
Upon completion of this activity, participants should be able to:
Disclosure Statements
The ACCP remains strongly committed to providing the best available evidence-based clinical information to participants of
this educational activity and requires an open disclosure of any potential conflict of interest identified by our faculty
members. It is not the intent of the ACCP to eliminate all situations of potential conflict of interest, but rather to enable
those who are working with the ACCP to recognize situations that may be subject to question by others. All disclosed conflicts
of interest are reviewed by the educational activity course director/chair, the Continuing Education Committee, or the Conflict
of Interest Review Committee to ensure that such situations are properly evaluated and, if necessary, resolved. The ACCP educational
standards pertaining to conflict of interest are intended to maintain the professional autonomy of the clinical experts inherent
in promoting a balanced presentation of science. Through our review process, all ACCP CME activities areensured of independent,
objective, scientifically balanced presentations of information. Disclosure of any or no relationships will be made available
on-site during all educational activities.
Disclosure of Unlabeled Use
In accordance with the ACCME Essential Areas and Policies relating to commercial support, the audience is advised that one
or more presentations in this continuing medical education activity may contain references to unlabeled or unapproved uses
of drugs or devises.
Disclaimer
The American College of Chest Physicians ("ACCP") and its officers, regents, executive committee members, members, related
entities, employees, representatives and other agents (collectively, "ACCP Parties") are not responsible in any capacity for,
do not warrant and expressly disclaim all liability for, any content whatsoever in any ACCP publication or other product (in
any medium) and the use or reliance on any such content, all such responsibility being solely that of the authors or the advertisers,
as the case may be. By way of example, without limiting the foregoing, this disclaimer of liability applies to the accuracy,
completeness, effectiveness, quality, appearance, ideas, or products, as the case may be, of or resulting from any statements,
references, articles, positions, claimed diagnosis, claimed possible treatments, services, or advertising, express or implied,
contained in any ACCP publication or other product. Furthermore, the content should not be considered medicaladvice and is
not intended to replace consultation with a qualified medical professional. Under no circumstances, including negligence,
shall any of the ACCP Parties be liable for any DIRECT, INDIRECT, INCIDENTAL, SPECIAL or CONSEQUENTIAL DAMAGES, or LOST PROFITS
that result from any of the foregoing, regardless of legal theory and whether or not claimant was advised of the possibility
of such damages.

This activity has been planned and implemented in accordance with the Essential Areas and Policies of the Accreditation Council for Continuing Medical Education (ACCME) through the sponsorship of the American College of Chest Physicians (ACCP).
The American College of Chest Physicians is accredited by the ACCME to provide continuing medical education for physicians.
The American College of Chest Physicians designates this educational activity for a maximum of 2.0 AMA PRA Category 1 Credit(s)
TM. Physicians should only claim credit commensurate with the extent of their participation in the activity. Anyone who attended
"Improving the Odds: Recognizing and Managing Complicated Infections in the ICU" session at CHEST 2007 when this content was presented, and already claimed CME for this presentation, cannot claim CME from this enduring product.
This product fulfills ACCP Learning Category II – Self Directed – Based Learning
For questions regarding the content of this activity, contact the accredited provider for this CME/CE activity noted above. For technical assistance, contact [email protected]
There are no fees for participating in or receiving credit for this online educational activity. For information on applicability
and acceptance of continuing education credit for this activity, please consult your professional licensing board.
This activity is designed to be completed within the time designated on the title page; physicians should claim only those
credits that reflect the time actually spent in the activity. To successfully earn credit, participants must complete the
activity online during the valid credit period that is noted on the title page.
Follow these steps to earn CME/CE credit*:
You may now view or print the certificate from your CME/CE Tracker. You may print the certificate but you cannot alter it.
Credits will be tallied in your CME/CE Tracker and archived for 6 years; at any point within this time period you can print
out the tally as well as the certificates by accessing "Edit Your Profile" at the top of your Medscape homepage.
*The credit that you receive is based on your user profile.
processing....
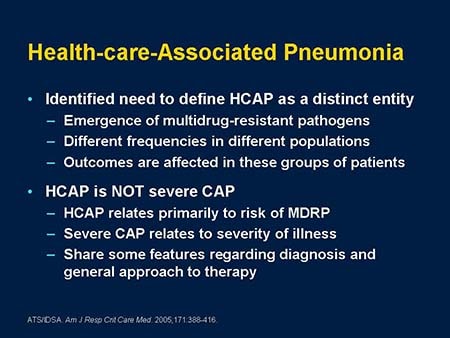
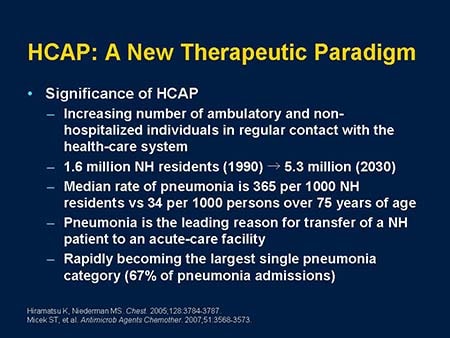
Marin H. Kollef, MD: My name is Marin Kollef. I am at Washington University in St. Louis where I am an intensivist. Lee Morrow is here from Creighton University where he is in the Pulmonary and Critical Care Division, and Lena Napolitano is Professor of Surgery at the University of Michigan and the Division Chief for Acute Care Surgery, Trauma and Burn Surgery as well. The first speaker is Dr. Lee Morrow who will be giving us some information on health-care-associated pneumonia (HCAP).